[04:46] [Damien Blenkinsopp]: Ben, welcome to the podcast.
[Ben Greenfield]: Hey, thanks for having me on man. And I’ve got to ask you, is it Damien, or Damion? Or Dami-something else?
[Damien Blenkinsopp]: Or Damian? It depends where you come from, I guess.
[Ben Greenfield]: Okay. Just checking. I don’t want to stick my foot in my mouth.
[Damien Blenkinsopp]: Yeah. You can call me Dam. I tell people to call me Dam, just to avoid all those questions.
[Ben Greenfield]: There we go. I want to sound like I’m cursing the entire episode.
[Damien Blenkinsopp]: Yeah. But it even works in Asia, tried and tested.
[Ben Greenfield]: Nice.
[Damien Blenkinsopp]: I mean you’ve got a three letter name. That works well.
[Ben Greenfield]: Yeah, totally. Ben.
(05:12) [Damien Blenkinsopp]: So, Ben, you’re into triathletes, Ironman, and basically the way I look at you is you go around searching for tactics and tools to give you an edge in these areas that you’re interested in. Is that a fair kind of back story to who you are and what you’re doing?
[Ben Greenfield]: Yeah, I do a lot of that I guess n=1 guinea-piging myself. Going out and doing crazy things like training with the Navy SEALS or doing these Spartan Races or Ironman triathlons, things like that.
But then I also think I learn just as much via a lot of the coaching and consulting that I do, just because people typically come to me for one of two reasons.
They either want to do some crazy feat that’s completely unnatural for the human body to do, like they want to go run 100 miles in the wilderness or something like that, and figure out how to do it without destroying themselves. So my job is to figure out how to do that from a nutrition and a physiology and an exercise standpoint.
Or they come to me because they basically want to live as long as freaking humanly possible, and want me to manage how do you sleep when you want to do something like that, how do you exercise, what do you measure, what do you pay attention to in your blood and your gut. And so there’s that kind of biohackiness that I get into.
And I’ve got to admit, for me personally it’s a little bit of both, really. I certainly do want to live as long as possible. I also want to do as many crazy events as I can during the process, see as much of the world as I can at the fastest pace possible. And so for myself, personally, I’m doing a little bit of both.
But sometimes people come to me and want to do something that I know nothing about, so I’ve got to go and learn it. So part of it is that, too. That, or if it’s not coaching someone it’s writing about that. Because I’ve done a lot of writing recently. This morning [I] published a big article on my website about how to use marijuana to get performance enhancing gains.
And I never really would have delved into that if I hadn’t been asked by so many people, especially here in the US with the growing legality. It’s like, can I use this while I’m exercising? That type of thing. So it’s a little bit of everything.
[07:12] [Damien Blenkinsopp]:Yeah, great. So [what was] the event that started the whole Ben Greenfield fitness podcast, and the blog and everything? How’d you get involved in that? Because you’re obviously very passionate about it.
[Ben Greenfield]: Yeah. Well there’s, I mean I get that question a lot, and frankly nothing against you but it annoys me, because I hate when people go, “When did you decide to do this? When did you decide to do that?” I never make decisions. I don’t have a 10 year business plan. I don’t have some ‘Come to Jesus’ moment where I said, “Oh hey, I want to learn how to exercise.”
It’s just that I live my life. I do things that I’m passionate about, or that other people who I’m helping are passionate about and tend to fall into whatever I might fall into based on that. I’m getting into hunting right now well specifically bow hunting and hunting competitions before that obstacle racing, before that Ironman Triathlon, before that water polo, before that body-building, before that I was a collegiate tennis player.
It’s just like life is a series of chapters and moving targets. It’s never just like one commitment to do one thing. But I would say, to give you a rough answer to your question, the very first time I decided to something a little bit more endurance orientated which I would define as something that has a nutrition rate.
You don’t see people dropping out of baseball or cricket games because of fatigue and heat stroke and lack of nutrition. That’s very rare, but you see it all the time in marathons and Ironman triathlons and things like that. So I would say the first time I started to get into that side of sports would have been my first Ironman Triathlon that I did back in the city of Portalane, Idaho in 2007.
And up until that point I’d been primarily an explosive power athlete. Like body-building and tennis and stuff like that. But my girlfriend, who is now my wife, was a runner. She ran cross-country for University of Idaho. So I kind of had to take up running, to a certain extent, just to be able to woo her.
And she dragged me to a triathlon one day and she actually had me run the running leg of the triathlon, which hurt like hell. I was a body builder; my boobs were bouncing up and down and my lower back was locking up and it was horrible. But it kind of got me interested in this high that you can get from endurance sports.
And so I wound up doing a few triathlons and doing, what I would say, is the biggest mistake for anyone who wants to avoid getting into endurance, that is I went and watched an Ironman Triathlon. And after watching Ironman and watching these intense feats of physical performance and the huge feeling of satisfaction and self-completion that these people were experiencing as they threw up their arms when they crossed the finish line I was like, I want that. I want to experience that.
And so I signed up for an Ironman and began taking everything I had been studying. At that point I had a Master’s Degree in Exercise Physiology and Nutrition and I was able to start applying that stuff to my training, and experimenting with a lot of what I was finding in research and sports science and seeing what worked and what doesn’t.
For example, all laboratory studies, or most of them, done by the white coats in their little labs will tell you that the body can take on about 200 to 250 calories of fuel during exercise. You can oxidize 200, 250 calories of carbohydrates while you are exercising. But for anyone, especially anyone who’s above about 150 pounds who has tried to go out and do an Ironman Triathlon, you completely bonk after about five hours on that number of calories, and you technically need about twice that in order to be able to get by in an Ironman race in most cases.
So, it’s a situation where what they’re saying in the lab and textbooks actually doesn’t work once you get out in real life and you try this stuff in the streets, in the trenches. So, that’s been kind of fun too, figuring out from research what works, and what doesn’t.
[Damien Blenkinsopp]: Right. Yeah, we often talk on here about n=1 experiments are often going to be different to the research, for a variety of reasons like the ones you brought up, and the use of averages, and other things like that.
[11:24] So, anyway, in terms of endurance training, since we’re there, what kind of biomarkers have you found to be the most useful to track your performance? Or what do you track around your capabilities for endurance training, and see as important?
[Ben Greenfield]: Oh, for endurance specifically?
[Damien Blenkinsopp]: Yeah.
[Ben Greenfield]: So for endurance specifically, that’s a great question. So one would be your level of HSCRP, which really that’s just for exercise in general. Or high sensitivity C-reative protein, just to make sure that your levels aren’t straying too high above 0.5. And the reason for that…
[Damien Blenkinsopp]: So that’s kind of your benchmark? You try to keep them under there? Where do yours tend to hover around?
[Ben Greenfield]: I actually fall below 0.2 now for HSCRP, probably because I eat a very anti-inflammatory diet, very clean. And I won’t insult your listeners’ intelligence by defining what a clean diet or an anti-inflammatory diet is, because it’s pretty easy to go out and figure that out with Dr. Google.
But I eat very clean. I also use a lot of anti-inflammatories. Like I make ginger tea, and I use a ton of turmeric, usually combined with black pepper to increase the efficacy of it, and I use percumin and I consume a lot of very dark and colorful vegetables with very limited amounts of dark and colorful fruits, and wild caught fish, and fats, and things that really help with inflammation.
And I’m also very careful with my training, where I do extremely focused and intense, but short, bouts of training with a specific purpose. I never go out and just pound the pavement for the hell of it, which is a great way to build up a lot of voluminous training based inflammation.
And so I have a very precise, dialed in training program that also includes things that help to mitigate inflammation, like foam rolling, and cold soaking, and these things that can help to remove a lot of these byproducts of metabolism that can create inflammation. So, inflammation is a biggie. Honestly, it doesn’t take a rocket scientist to figure out that if you keep your inflammation controlled, it’s a good thing.
So, a few others that I’ll pay attention to for endurance. When we’re talking about labs, as far as blood goes, TSH, preferably a full thyroid panel, is pretty prudent to pay attention to simply because high level endurance training can inhibit conversion of inactive to active thyroid hormone.
And because of the high amounts of cortisol that can potentially be produced through an improper training program can stress the body out enough to where you experience some hypothalamic pituitary adrenal axis insufficiencies, particularly high cortisol, creating a feedback loop that reduces the conversion of inactive to active thyroid hormone and thus an increase in thyroid stimulating hormone. So your body turns out a bunch more thyroid stimulating hormone to try and get more T4 present, even though a lot of that T4 isn’t getting converted into T3.
And by monitoring TSH, if you see a pattern or a rise in TSH many times it’s concomitant with an increase in cortisol and stress, and often also accompanies a not enough eating period. Sometimes not enough carbohydrates is the biggest culprit, but in many cases just not enough damn calories, period. Damn, not referring to your first name but to the curse word. Just so we’re clear.
That’s another one is TSH. Cortisol, I alluded to, but when we’re looking at a hormonal panel, I also like to pay attention to sex hormone binding globulin. Because the body has this interesting mechanism where when it’s stressed out, when it’s in a time of famine, in a time of need, under high amounts of stress, doing a lot of migrating, a lot of moving with low amount of calorie intake, the last thing you want the body to do is produce a bunch of babies at that point.
And so sex hormone binding globulin often rises simultaneous to cortisol to keep total testosterone bound, and keep it from being available as free testosterone. So even if your testes are working just fine, or your pituitary gland is working just fine, obviously talking about the males more than the females now and even the leydig cells in your testes are producing testosterone just fine, if sex hormone binding globulin levels are really, really high that’s all for naught. And so that’s another really, really important one to keep an eye on. And that’s typically addressed by addressing cortisol.
[15:50][Damien Blenkinsopp]: Right. So, why would you look at SHBG versus free testosterone, or that marker? The [unclear 15:56]?
[Ben Greenfield]: Well, because if free testosterone is low, but if you look upstream perhaps it’s because total testosterone is low because the leydig cells in your testes are not producing enough hormone because you’ve got low levels of luteinizing hormone. In contrast to that, perhaps your luteinizing hormone production is fine, your leydig cells are producing enough testosterone just fine, your total testosterone is high, but it’s more of a cortisol issue than it is a central nervous system issue or a glandular issue.
So that’s why you test that versus just looking at free testosterone.
[Damien Blenkinsopp]: So basically, free testosterone could be many, there’s more reasons behind it, but the SHBG is more specific to endurance and specific dynamic.
[Ben Greenfield]: Yeah. Really, two reasons behind it. Either you aren’t producing enough total testosterone, or you are producing enough total testosterone but it’s not getting converted. So those are really the two main things to look at.
[16:48] [Damien Blenkinsopp]: So, are you looking at the standard reference ranges for that, or do you look for something a bit more precise?
[Ben Greenfield]: A lot of times you have to look at symptoms synonymous, because standard reference ranges are going to vary widely.
I’ve worked with a lot of endurance athletes who have very high libido levels, show no signs of over-training, have very robust nervous systems, high heart rate variability, low cortisol, and even low sex hormone binding globulin, but their total testosterone is in like the high 300s. Which, for a body builder they would scoff at that and say, oh that’s rock bottom low. Even though a lot of times hypogonadism is levels below 100.
And you’ll get many people who just feel like fricking crap at 300, and some people will be closer to 500, and some people will need levels of 700, 800, or even 1000. So it kind of depends. It varies widely, I suspect based on genetics as a big part of it.
So ultimately it’s really tough to hold things up to reference ranges. I mean, you can ballpark it. You can say well if total testosterone is starting to get below 300, that’s where we would really start to get a little bit concerned. But it really is kind of tough. A lot of times it’s a moving target based off of a cluster of other symptoms.
If someone’s complaining of low libido and low motivation, and lack of energy, etc, and their testosterone is at 400, well that’s a pretty good sign that 400 is not going to be adequate for them. So I know that’s one of those deals where it’s total soft science, but it does really depend. That’s one of those ‘it depends’ answers, but that is definitely a variable that I will look at.
[18:20] Liver enzymes is another one, like alkaline phosphatase, aspartate aminotransferase, the ALT, the AST, some of these liver markers just because a lot of times they can be elevated when excessive exercise is present. And so that’s another one to pay attention to. It doesn’t have to be excessive exercise; sometimes it can be alcohol, pharmaceutical intake, things of that nature. But liver enzymes are the one that I’ll look at.
Kidneys, a lot of people say to look at kidneys, but frankly it’s very rare for me to see an athlete who doesn’t have slightly elevate creatinine and blood urea nitrogen levels, which are two common markers in the kidneys that a physician will get concerned about if they see elevated, but that are very common to see elevated if an athlete is exercising anywhere in the 48 hours leading up to a blood panel.
So, as long as creatinine levels aren’t much higher than about 1.1, and as long as blood urea nitrogen isn’t through the roof and I apologize, but off the top of my head I don’t remember the lab reference ranges for blood urea nitrogen. The reason being that I do most of my coaching for blood panels with a company called WellnessFX. It’s basically more like a dashboard with graphs, more than it is hard numbers, so occasionally I’m looking at graphs more than I am numbers.
[Damien Blenkinsopp]: And they just have those red zones.
[Ben Greenfield]: Yeah, exactly. They’ve got red, yellow, green, which actually annoys me some of the time. Because they’ll flag high LDL as red when I purposefully try to get my LDL high. So there’s some issues with the whole red yellow green type of quantification. But anyways, blood urea nitrogen and creatinine, even though a lot of people talk about those, they’re not super duper important in my opinion, because they’re always going to be a little bit elevated.
Vitamin D, that’s another one that I’ll look at just because of it’s importance. As you can suspect, a lot of these aren’t just specific to endurance, they’re specific to exercising period. Just as a hormone and a steroid, vitamin D is another important one that I’ll look at.
And then as far as other things, I typically will have most of the athletes I work with or the people I advise do at least once a year a full gut panel. You know, a comprehensive gut panel that includes parasitology, measurement of pancreatic enzyme production, measurement of yeast and fungus and any type of bacterial overgrowth in the digestive tract because I find that, especially when you’re jogging your body up and down for 10 plus hours while racing, having a really, really good gut and GI system and very efficient digestion is incredibly important.
And so I will look at things like presence of yeast or fungus, like Candida Albicans, or the presence of H pylori, or absence of hydrochloric acid, or absence of pancreatic enzymes, or overgrowth of specific bacteria, or lack of short chain fatty acids in the digestive tract, in the colon, and a lot of those things that tend to influence an athletes performance or their feelings of well-being. So that’s another thing I’ll pay attention to.
[21:18][Damien Blenkinsopp]: Right. A lot of people wouldn’t think of that as something performance related, more like a chronic issue related.
Have you got any case studies where you saw people, basically not performing but not having any negative symptoms in terms of GI distress or anything that they would have noticed, but when you put through these tests some negative results came?
[Ben Greenfield]: Sure. Now we’re delving a little bit more deeply. And I mean, obviously explosive diarrhea halfway through a marathon can be a good sign of digestive enzyme insufficiency, but so can, for example, vitamin B12 or vitamin D deficiencies, or even if you go more advanced and run like an organic acids profile, or an amino acid profile, severe imbalances of a lot of micro-nutrients.
Well if you’re not digesting your food efficiently, for example, if you’re not producing adequate hydrochloric acid, you’re not activating pepsin to break down proteins, beginning in the stomach an moving on to the small intestine, then you’re going to: a. have undigested protein fragments winding up in the bloodstream causing some auto-immune issues, and that can include fuzzy thinking, which no athlete wants.
But then you also can get amino acid deficiencies, like deficiency in the ability to create neurotransmitters, and also deficiencies in the ability to repair and regenerate skeletal muscle tissue, because you aren’t breaking down the proteins that you’re eating.
And the same could be said for something like inflammation in the digestive tract from wearing down of the microvilli. So perhaps you’re not producing adequate levels of lactase, so you’ve got some lactose issues and bloating and gas. Or you’ve got inflammation that is resulting in malabsorption of fat-soluble vitamins, so vitamins A, D, E, and K aren’t getting absorbed properly, or bacteria aren’t helping you to produce those, and so you experience hormonal deficiencies, or steroid deficiencies.
And so, yeah the gut is incredibly important, and that’s one of the things I’ve been kind of getting on companies like WellnessFX, for example, to do is to not just use the strategy of blood testing but also really pay attention to the gut. I mean, in an ideal scenario, what I would like to see is a done-for-you system.
And for me right now, what I do is just kind of string this together for the athletes who I work with. But a done-for-you system where you get your blood testing, you get your gut testing, and you get your genetic testing so we can look at everything from genetic snips to bacterial imbalances in the gut to all the blood and biomarkers, and have all of that done with either one panel or one service.
That would be really nice, because right now you’ve got to go to typically three different places. You’ve got to go to whatever DNAFit, or 23andMe, and you’ve got to go to DirectLabs, or Metametrix for GI affects, and then you’ve got to go to WellnessFX for whatever else. And then if you want to do food allergy testing, well then you’ve got to throw in a Cyrex panel, or something like that.
So maybe it’s a first world problem to want all this stuff to be available in one central location, but it certainly would be nice.
[Damien Blenkinsopp]: Yeah. It’s so near the early days from that perspective. There’s a lot of specialized, it’s still kind of specialized in terms of the labs. Each is in their little separate box and everything.
[Ben Greenfield]: Yeah.
[24:17] [Damien Blenkinsopp]: So, in terms of the kinds of decisions you’ve made, or you’ve advised a client based on some of these values, some of this data that’s come back, what have been the biggest changes that you’ve implemented to optimize training?
[Ben Greenfield]: You mean as far as training?
[Damien Blenkinsopp]: So, say the TSH came up too high, what would you do about that?
[Ben Greenfield]: Oh okay, so for high TSH, obviously it’s never a shotgun approach. It’s never a multivitamin. So for high TSH it may be looking at your carbohydrate intake. That’s the first thing that I’ll look at.
Even before you look at total amount of calories, you just make sure nobody is on some low, like 40 gram per day carbohydrate diet, because frankly a lot of the ‘low carb’ or ‘ketosis’ based diets that are out there were created for sedentary people. Even the bulletproof diet. I love the whole bulletproof philosophy, but it was written by a computer programmer, not by an athlete.
And so the levels of carbohydrate, and even the levels of calories in that diet, have to be adjusted and modified for a hard-charging athlete, especially an endurance athlete. So, otherwise with caloric depletion and carbohydrate depletion, you basically lose a lot of your ability to convert inactive to active thyroid hormone.
And in the case of calories, as you would deduce through common sense, when you send your body a message that calories are insufficient but you’re still requiring it to move a lot, your body down regulates metabolism. And one of the main ways it does that is by down regulating thyroid.
So, I look at carbohydrates, I look at calories, and then I also look at dietary intake of organ meats and fat soluble vitamins, which can also assist with thyroid health. So in my case, because I did an n=1 experiment about a year and a half ago where I did 12 months of ketosis.
Not cyclic ketosis, not cycling carbohydrates in and out throughout the day, but full on eating only 5-10 percent of my total daily intake from carbohydrates. Very low carbohydrate diet. Too low, in my opinion, for most endurance athletes who want to maintain optimal levels of health elsewhere.
[26:10] [Damien Blenkinsopp]: Did you see negative effects from that over the 12 months?
[Ben Greenfield]: Yeah, and that’s what I’m getting at with the thyroid. I started taking thyroid glandular extract. I took one called Thryo-Gold, which is made from New Zealand cows, that are like an A2 cattle.
A lot of A1 cattle has proteins in it that cause an immune reaction within the human body, but cattle that are breed via A2 are cattle that contain this A2 genetic profile that is more bio-compatible with the human body. And so I basically took a T1, T2, T3, and T4 combo, and that seemed to turn my thyroid around. But that was after I had already done a number on it.
So for thyroid, that would be an example of what I would do with something like thyroid, would be increase calories, increase carbohydrates, increase intake of organ meats and fat soluble vitamins. And then for a really hard-charging athlete who insists upon doing something like restricting carbohydrates to tap into the performance enhancing effects of ketosis, understand that you’ve got to get on extra help from the thyroid.
Since your body isn’t going to make T3, dump it into the body. And preferably get it from a whole source, like levothyroxine or synthroid. But a source that contains other elements of thyroid in addition to just T3, so you’re not creating an imbalance.
[27:22] [Damien Blenkinsopp]: Great. Well, connected with the thyroid issues, I was wondering if you’ve come across adrenal fatigue also. If that’s every come up with you or with anyone else.
[Ben Greenfield]: Absolutely. Adrenal fatigue, gosh. There’s like four chapters of my book on that alone. But adrenal fatigue, well what do you want to know about it?
[Damien Blenkinsopp]: Well first of all, have you looked at some of the tests? I’ve done some of the salivary tests.
[Ben Greenfield]: Oh yeah. Yeah, like an adrenal stress index is kind of gold standard, cortisol DHA. If you look at the cortisol DHA curve, that’s much, much better when you’re addressing something like adrenal fatigue versus a blood cortisol measurement, which is just a snapshot. You want to see a moving target of salivary cortisol levels, preferably matched to salivary DHEA levels, throughout the day.
[28:03][Damien Blenkinsopp]: I was just thinking, based on it’s endurance exercise, and it has this tendency to raise cortisol, that that would be more of an issue and something that you would keep an eye on. Or by monitoring TSH, does that kind of take care of itself? If the TSH is alright then you tend not to have an adrenal issue as well?
[Ben Greenfield]: No, not necessarily.
You can still have adrenal fatigue and have a thyroid that’s managed properly. Because what you would typically see in that case is someone is eating boatloads of calories and taking care of themselves from an energetic standpoint, but simply outputting too much energy. They’re just training way too much. Even though they’re supplying their thyroid with what it needs, there’s just too much training still.
And a lot of times you’ll see inflammation high, but yeah. Cortisol DHEA, and that adrenal stress index can be a good measurement. And there are less quantitative measurements. You could do a pulst test, where you look in a mirror and you shine a bright light at your eyes, and your pupils should stay dilated. But if it stays dilated and then just starts flickering rapidly.
[Damien Blenkinsopp]: Have you tried that one?
[Ben Greenfield]: I have, yeah.
[Damien Blenkinsopp]: Because I was just wondering. I did try it and I find it a little bit difficult to judge.
[Ben Greenfield]: Yeah, it’s certainly not as precise as a salivary measurement, but once you’ve done it a few times you can definitely see the pupil, and whether or not it’s actually flickering versus staying dilated. If you look at if for long enough, it’s just going to start flickering period, but if it starts flickering after just a few seconds, that’s typically a sign that your kidneys are not producing enough aldosterone, which is synonymous, or can accompany, adrenal fatigue.
The other one is just the dizziness test. If you lay down or you sit down and you stand up quickly and you get dizzy, that can be a sign of blood pressure mismanagement that often goes hand-in-hand with adrenal fatigue. And again, these are the super cheapo poor man’s methods, but it can give you clues.
And then there’s temperature tests for thyroid, the Broda Barnes Temperature Test, where you do oral and axillary measurements of your temperature in bed every morning, and keep a running graph. And if it’s consistently low, that can be a pretty good indication that even if you haven’t done a blood thyroid test that your thyroid might be having issues.
So, there are a lot of things. One of the best ones I like though is just pure heart-rate variability. Testing the interplay between your sympathetic and your parasympathetic nervous system by using something like a Bluetooth enabled heart rate monitor and one of these heart rate variability apps, and simply paying attention to whether heart rate variability is high or low on any given day.
And if it’s consistently low, and you see consistent suppression of both sympathetic and parasympathetic nervous system feedback, then that can be a pretty good sign that you’re on the cusp of adrenal fatigue illness or injury, and so that’s another really good one to pay attention to. And I do that one every day myself.
[Damien Blenkinsopp]: Do you do it in the morning as soon as you wake up?
[Ben Greenfield]: Yes, that’s gold standard, because that’s where most of the studies have been done on heart rate variability were five minutes resting in the morning.
[30:45] [Damien Blenkinsopp]: Right, right. I believe you use the HR…what’s the name of the company?
[Ben Greenfield]: SweetBeat?
[Damien Blenkinsopp]: Yeah, SweetBeat.
[Ben Greenfield]: Yeah, but because I want to build up that technology and add some features and stuff like that, I’ve actually white labeled their technology. And so I use the app called NatureBeat now, but it’s the SweetBeat technology.
[Damien Blenkinsopp]: Great, great. Yeah, she’s been on the show.
[Ben Greenfield]: Yeah.
[Damien Blenkinsopp]: So I was using that for a long time, and then I just recently started using iFleet, because I also talked to the guys at iFleet, and it does have this other thing that they just added recently. You might just want to check out.
It’s kind of interesting. It shows how high your energy levels are on a given day, so it kind of does this matrix thing. So it shows you if your in the bottom right corner, it means something a little bit different. So I’ve been checking it out. I’m still trying to understand what it means each day. But I do find that when I’m at the bottom, low energy, those days tend not to be good. Even if I have a high HRV.
[31:39] So anyway, out of interest, what is your HRV levels? Because you think normally endurance athletes have higher HRV, right?
[Ben Greenfield]: Yeah. Usually higher HRV, which isn’t necessarily a good thing if you’ve got what are called HF to LF ratio imbalances.
You want your HF to LF ratio to be pretty close to one. That’s sympathetic and parasympathetic nervous system feedback. And if parasympathetic nervous system feedback, which would be your high frequency number, if that’s super duper depressed, and your LF is really high that can be an indication of aerobic based over-training, or vice versa.
So ideally you’ve got high HRV and a pretty close to a 1-1 ration between HF and LF. That’s what you want to go to. And you want both HF and LF to be up in the thousands. That’s a sign of a really robust nervous system.
So, my values tend to be between about 92 and 98, with HF and LF values that vary between about 4,000 to 8,000, around in there. Generally with a 1-1 ratio, depending on what my previous day’s training had looked like.
And I would expect, for example, this Tuesday I’ll do a CrossFit’s Murph and I’ll do that with a 20 pound weighted vest on, and just crush myself. And that will take me about an hour to do, and I guarantee my LF value will be tanked the next day. But I also won’t be doing any sympathetic nervous system training for like 48 hours afterward.
[Damien Blenkinsopp]: So you recover within 48 hours?
[Ben Greenfield]: 48 to 72 hours, depending.
[Damien Blenkinsopp]: These scores recover for you pretty quickly?
[Ben Greenfield]: Yeah, but I mean, if I were to do something epic, right? Like, usually something that gets you to the state of glycogen depletion. Or let’s say instead of Murph, I do double Murph, or I do a Murph with a 5k sandwiched on either end rather than just a mile, then it can take me several days to recover, for sure.
[33:23] [Damien Blenkinsopp]: If you had to pick one marker to optimize your endurance training by and make decisions on, which one of the ones we’ve talked about would it be?
[Ben Greenfield]: HRV.
[Damien Blenkinsopp]: Okay, great.
[Ben Greenfield]: Just because it’s easy, right? You don’t have to give blood.
And maybe at some point, once we’ve got the lab and chip technology finalized, and I can put a drop of blood onto a little dongle that will plug into my iPhone and I can measure, let’s say, testosterone cortisol ratios, maybe that will become a more valuable metric for me. But at this point, I would have to say something simple and easy to utilize and relatively inexpensive, the HRV would be the one that I’d choose.
If I had to choose an actual blood biomarker, tough to say. Tough to say. I guess I’d probably have to go with HSCRP, again. Just because inflammation is generally going to be high when cortisol is high. It’s generally going to be high when diet is crappy, it’s going to be high when triglycerides are high, it’s going to be high when omega-3 fatty acids are low. So, that’s a pretty good one to measure.
[Damien Blenkinsopp]: Yeah. So it catches a lot of things. Mainly whenever something starts going wrong.
[Ben Greenfield]: Yeah.
[34:29] [Damien Blenkinsopp]: Well so you’ve referred to over training quite a bit over this as something that you’d have to change. So HRV would be one of the first places you’d see over training.
Are there any other tell-tale markers, and what do you suggest, more to the point, because you mentioned earlier that you do very is it short, intense kind of endurance exercises. And I think a lot of people when they’re thinking about endurance, they’re thinking about very high-volume, kind of long duration activity.
So how do you approach it, and avoid over training? What are the top things you’ve taken in over time?
[Ben Greenfield]: First of all, one of the common pitfalls that people fall into with endurance training is doing the long voluminous training every weekend. It’s very stereotypical that you’ll see in a lot of athletes these Saturday long bike rides and then Sunday long run, for example. Or in a marathon, the Saturday long run.
I’ve found that in most cases, you can maintain endurance really, really well. Unless you’re a professional athlete trying to perform at the peak of performance, most people can perform just fine. With doing digging into the well like that, really, really, deep for like a death march, a really long ride or something like that, you typically only need to do that one to two times a month. Not every weekend.
I’m a bigger fan of using shorter, very temporal based intervals. So to give you an example, for the Ironman triathletes that I work with, while their peers are out doing a five hour ride followed by an hour long run, my athletes will be doing two hours of 20 minutes at race pace followed by 5 minutes recovery. So a very focused activity with a specific goal in mind. And then they’ll finish that up with a 15 minute tempo run at a cadence of 90 plus.
So it’s all extremely high quality. And then once a month they’ll go out and do something big, something long, something voluminous that builds the mental tolerance to training, but that doesn’t dig so deep into the well as doing it every week.
And the reason for that is based off of the human body’s natural slow twitch muscle fibers. The human body’s ability to cool because we’re upright and not covered in fur and hair. Our ability to sweat, rather than pant, to reduce heat. And a cluster of other factors.
We’re pretty good at going for long periods of time. And when training for endurance, bigger limiters are things like power, speed, cadence, strength, the integrity of the fascia connective tissue, the intelligence to be able to use nutrients and calories properly.
And really pointing in one direction, and going for long periods of time is not that much of a weakness for the human body, but the problem is that it’s easy. And people take pride in it. They’re like, “Oh I persevered today. I did my three hour run.”
And my question to you is well yea, but what did you accomplish side from being on your feet for long periods of time? Which frankly I could stand up at my standing workstation and write an article for three hours and get the same amount of time on my feet as you just did out pounding the pavement. So it would be better in that case to do something with intervals at race pace for a shorter period of time.
Focus on cadence. Allow enough time before and after for a good warmup. Maybe some meditation and breath work. Some good recovery. And so that’s where the more intense, more quality, lower volume approach nine times out of ten trumps the voluminous approach.
The exception to that fact would be the person who has a lot of time on their hands to train: the professional athlete. Professional athletes, assuming they’re using this 80-20 approach, it’s called polarized training. 80 percent of your training is done aerobically, with about 20 percent done high intensity.
That approach works very well, and it is what a lot of the elite cross-country skiers and marathoners and cyclists etc. will use, but what is important to understand about that approach is it requires many, many hours per day.
That approach can require two to four hours per day of training, and even more than that, on weekends, for example. And the majority of folks simply don’t have the luxury of time available to utilize that approach effectively. That in a nut shell is my approach to training.
I’ve got a couple of athletes who I work with who are more, what I would consider to be on the professional level, who have that luxury of time. And I do train them with that aerobic approach, where they’re out doing long voluminous sets of training at a controlled heart rate aerobically, putting lots of time in the saddle or time on the pavement. But its very few and far between that I’ll recommend an athlete to train like that.
[Damien Blenkinsopp]: Great, great, thanks. That’s a great summary of it.
[39:01] I wanted to move on to, because I know you did this 12 months of ketogenic dieting. Could you talk a little bit about that? Give us an overview. What was your approach to that, what were you actually eating, and was there any specific goals to track over the year?
[Ben Greenfield]: Well yeah, for that specific diet, that was for a study at University of Connecticut that was done on, basically, a group of athletes who followed a high-carb/low-fat diet, versus a group of athletes who followed a high-fat/low-carb diet.
And it was basically a measurement of fat oxidation during exercise. And they also did muscle biopsies before and after exercise to see the rate of glycogen use as well as the rate of glycogen replenishment following the post work out meal to just see if the body does a better job at oxidizing fat, or at sparing glycogen during exercise when you’ve eaten a high-fat diet.
And it did turn out in that study that the athletes who followed the high-fat diet were oxidizing a lot of fat. The textbooks tell you that you can burn about 1.0 grams of fat per minute, and the group of athletes who followed the high-fat diet were burning 1.5, 1.6, 1.7 grams of fat per minute. Literally rewriting the textbooks when it comes to how much fat you can burn during exercise.
I haven’t seen the muscle biopsy data yet to see how much glycogen conservation actually took place, or whether or not the body became more glycogen depleted when using primarily fatty acids as a fuel. But ultimately, what that diet consisted of was really controlling carbohydrates.
Whereas I would normally and this is what I do now I would carb-cycle, or I would do cyclic-ketogensis or cyclic-ketosis, where I don’t eat carbohydrates all day long and at the very end of the day, typically in the post-workout scenario, with dinner I’ll eat anywhere from 75 to 200 grams of white rice, red wine, sweet potatoes, sourdough bread. You know, safe starches, not like pizza and ice cream, but good carbohydrates. And then the rest of the day just high fat and moderate protein.
Whereas on this full on ketosis diet, it was pretty much just things like bulletproof coffee, and high fat shakes and lots of coconut milk and coconut oil, and heavy cream and MCT oil and seeds and nuts, and just fats, fat, fats. Bone broth and avocados, and olives, and you name it.
And frankly, in my opinion, it wasn’t that enjoyable to have to not have sweet potato fries, and not have, even coconut ice cream has cane sugar in it. So you have to make your own with chocolate stevia. And so it’s a little bit laborious and a little bit tough, but I mean at the same time the endurance payoff was huge.
The amount of focus that I had for long periods of time. My ability to just hop on a bike and ride for hours with no fuel at all, with just water. It was pretty profound, because you produce all these ketones as a bi-product of fatty acid oxidation, and they’re used as the preferred fuel by the brain, by the heart, by the liver, by the diaphragm while you’re out exercising. And that’s a huge boon to an endurance athlete.
And like I mentioned, there’s some blow-back. Like the TSH could take a hit, the testosterone could take a hit. But ultimately, it’s a cool little bio-hack. If I could go back and do it over again, I would definitely start taking thyroid glandular earlier to stave off some of those thyroid issues.
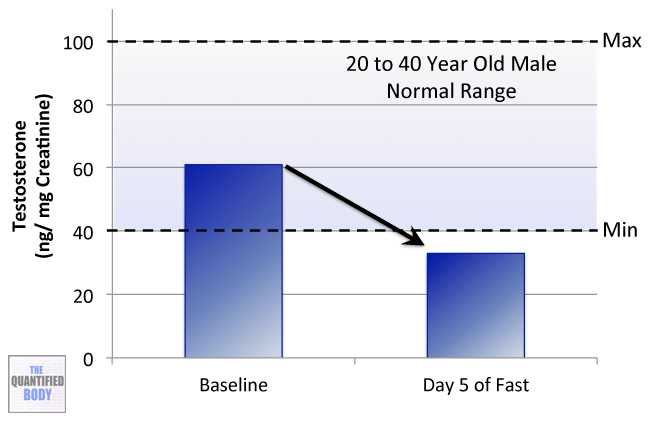
I would, it’s not legal but I would really encourage folks to pay attention to testosterone. And I mean like, you can’t use testosterone in a WADA, or a USADA or like an NCAA sanctioned event, but my testosterone dropped so much during that experiment with ketosis, I would say if you’re not competing, use AndroGel or just some kind of testosterone support because your testosterone is going to fall to pieces.
And then the question becomes well is it really worth it to you if you’re doing this thing and you’re not even competing.
[Damien Blenkinsopp]: Yeah. Did you feel different?
[Ben Greenfield]: Oh, yeah.
[Damien Blenkinsopp]: Because we talk about testosterone with things like anxiety, your drive, your libido, of course. And so did you get any kind of low testosterone symptoms?
[Ben Greenfield]: Oh yeah. Absolutely. I mean even something as simple as only having to shave every four or five days, whereas normally I would just shave every one to two days.
[Damien Blenkinsopp]: That’s a benefit.
[Ben Greenfield]: I mean, little things like that, but you notice. Yeah, potentially. You save money on razors.
Yeah, the libido, sex drive, number of times having sex per week, desire to have sex, quality of the erection, all of those kind of things certainly they took a hit during ketosis. They weren’t good. But that was, mind you, ketosis in the presence of high amounts of physical activity. Even doing the ‘low volume approach’ it’s still a massive amount of work, right?
[Damien Blenkinsopp]: Right.
[Ben Greenfield]: You’re still working out 60 to 90 plus minutes every day, and longer than that on the weekends.
And you look at something like Dr. Terry Wahls and her ketosis approach for managing MS. Well sure. I mean, that’s going to work just fine for managing MS. I mean, going on a walk with your dog every morning, and maybe lifting easy weights, three sets of 10 for 20 minutes twice a week.
But once you jump into hard exercise, it’s a whole different type of ketosis.
[Damien Blenkinsopp]: Right, right. Just to be clear, were you getting better times? Did you feel like you were competing better?
[Ben Greenfield]: Oh, I was competing way better. Yeah. Absolutely.
[Damien Blenkinsopp]: Right. But it’s just the downsides to your lifestyle, to all the other things, were too great to do this on a constant basis.
[Ben Greenfield]: In my opinion, yes, because I don’t like being cold all the time, I don’t like not having libido. So again, I’m not saying you can’t do it properly, even though it’s way, way tougher once you get into training, but I think that you basically have to use supplementation pretty intensively.
[44:34] [Damien Blenkinsopp]: Did you kind of see the benefits evolve and get much better as the months passed, or is this something someone could do on a month basis, one month on and one month off?
[Ben Greenfield]: For exercise, you barely even see any benefits until you’ve been doing it consistently for about six months, and the real benefits start to manifest after one to two years.
But the other thing to realize is that right about the time I finished up the experiment, companies like KetoForce started coming out with beta hydroxybutyrate salts that could be consumed to elevate your ketone bodies, even in the presence of a lot of carbohydrates or glucose. And so it’s possible that now, since the experiment that I did, you could get the best of both worlds.
And I actually have some bottles of the beta hydroxybutyrate salts and the resistance starches, and a lot of the things that, if I had to go back and do it all over again, I would try to get the best of both worlds. I would eat more carbohydrates, but then I would also hack myself into ketosis by consuming actual ketones bodies.
The question there becomes a matter of long term health and gut health and how that actually manifests in terms of actual symptoms or the way you felt, or even I would definitely pay close attention to blood and biomarkers.
Were I to delve into that type of bio-hack? I potentially may. I could see myself, and obviously I’m at a point in my athletic career where I’ve still got a good eight years of hardcore performance left in my body, and I could see one of those years being spent utilizing a ketonic approach again, but with the incorporation of beta hydroxybutyrate salts, resistance starches, even higher amounts of MCT oils, particularly like the C8s and the C10s. And a little bit more attention paid to ways to get into ketosis that go above and beyond just carbohydrate restriction and exercise.
[Damien Blenkinsopp]: This is great Ben, this is a wealth of information.
[46:20] In terms of the biomarkers you would track, you said you would track some biomarkers if you were going to do this again what kinds of ones that we haven’t spoken about already would you look at? Did you track your blood ketones?
[Ben Greenfield]: Yeah. Breath ketones. I mean, urinary ketones become, many times, absent after a few weeks in ketosis just because you’re utilizing your ketones. Blood ketones are accurate but expensive and invasive to test, and breath ketones are pretty [easy].
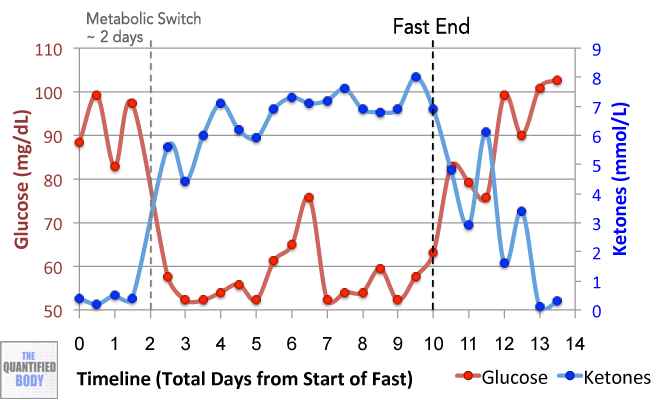
There are breath testing monitors like the Ketonix device that, one breath and you know your ketones, and you’re good. So breath testing is a really good way to go as far as measurement of ketones. You look for values anywhere from 1.0 up to 3.0 millimolars. You’ll finish exercise as high as 7.0 millimolars.
You’ll rarely see ketoacidosis, which would be like 10 plus millimolars. It is a non-issue. I have yet to see any athlete I work with go under ketoacidosis, which would be an actual deleterious biological state. Not something you need to worry about unless you are letting yourself become severely hypoglycemic.
[47:20] [Damien Blenkinsopp]: So again, is that something you saw evolve over the months? Like your ketones ratings would get higher.
[Ben Greenfield]: Yeah. You get to the point where it’s just super duper easy to get into ketosis. Yeah. And your ability to go for long periods of time without eating just goes through the roof.
So ultimately, the biomarker I would say, in addition to what we’ve already talked about, would be breath ketones. And then pay attention to triglycerides too, because they’ve shown that compared to total cholesterol values, a better predictor of your coronary disease risk factors is your triglyceride to HDL ratio, specifically keeping that at one or lower in terms of your number of triglycerides versus HDL.
But I’ve found that some people will switch to a high-fat diet and have such a high intake of vegetable oils, and even an imbalanced high intake of animal based oils, like butter for example, versus olive oil and avocados. Their triglycerides go through the roof.
Pay attention to that HDL ratio. That’s my advice is make sure that that thing isn’t getting much above one, that would be another important thing to pay attention to, especially on a higher fat intake.
[Damien Blenkinsopp]: Great, great. Excellent points.
[48:25] So there are a couple of other things I’ve noticed you’ve done in your experiment. I read your book of course. One of the things that we’ve come across before I spoke to Alan Cash from benaGene oxaloacetate, and I was wondering what you’ve done with that and if you’ve tracked anything or learned anything about that.
[Ben Greenfield]: Yeah, obviously if you talked to Alan Cash your listeners can go back and listen to that to learn more about what oxaloacetate is. But in a nutshell, the reason that I used it was because it can increase the turnover rate of lactic acid into pyruvate, and increase the rate at which lactic acid is shuttled back up into the liver to be reconverted into glucose.
And so if you are eating a low-carbohydrate diet anyways, that by nature means you might not be taking as much exogenous glucose in, or might not even have as high a level of glycogen stores, but you can still take the lactic acid that you’re producing as a byproduct of metabolic activity anyways and have that reconverted into usable glucose sources to have a glycogen sparing effect and to get a little bit more intensity. And so the way that would be achieved if you’re going to increase the rate of that cycle, which is called the Cori cycle, would be via the use of oxaloacetate.
And so, I actually did use that. I don’t use it right now. It’s one of those things where it’s just like, I would benefit from it its just one more supplement to remember to take. But I certainly used it through that entire ketotic experiment with the oxaloacetate just to increase the conversion of lactic acid into glucose.
[Damien Blenkinsopp]: Right, it sounds like it would help specifically in that ketogenic diet state when you’re exercising.
[Ben Greenfield]: Exactly.
[Damien Blenkinsopp]: So you designed it that way? You decided to take it before, or was it something you came up with afterward to help?
[Ben Greenfield]: I talked to Alan at one of the Bulletproof bio-hacking conferences. We talked about the physiology of oxaloacetate, and then based on that I just kind of had a little light bulb moment, where I realized that if I was restricting carbohydrates anyway, that this was one more way that I could create endogenous glucose more quickly.
[Damien Blenkinsopp]: Great, great.
[50:27] Cold thermogenesis. Do you still play around with that? Is there anything like, for instance, have you seen your HSCRP any time, potentially when you first started it or did it a bit more intensively, change with that?
[Ben Greenfield]: Yes. I have not done a dedicated experiment with cold water exposure, cold temperature exposure, or the use of ice baths or cold showers to see the direct effects on HSCRP, although reduction of inflammatory cytokines has been observed in literature when it comes to cold thermogenesis and inflammation.
What I use cold thermogenesis for is increased conversion of white adipose tissue to brown adipose tissue. Simply because it’s very difficult to kill fat cells, but you can convert fat cells into energy utilizing and heat producing tissue. And that’s one thing that cold thermogenesis is good for. That would mean cold baths, cold showers, cold soaks, etc.
Also very useful for increased production of endothelial nitric oxide synthase, which can cause your blood vessels to dilate much more readily, which is good for everything from exercise to sex to heating your body when it needs to be heated. And then there’s also increased tolerance to the mammalian dive reflex, which is that activation of our sympathetic fight-or-light nervous system in response to stress.
And when you are able to withstand cold stress without taking that sharp influx of breath, that means that you have become more resilient and more resistant to subconscious activation of that fight-or-flight nervous system. You’re better at controlling stressful events that happen.
And so, what I do is I never take a warm shower. I do a cold shower in the morning, cold shower in the evening. I do once per week a 30 minute cold soak that gets me up to shivering level, typically needing to shiver for one to two hours afterward in order to regain warmth. And those are the ways that I use cold thermogenesis. I also keep my house relatively cold. My office is at about 55 degrees. In my home, typically I’ll sleep at 60 to 65 degrees.
It’s just a really, really good way to make yourself tough, to burn fat, and to increase blood vessel health. And it’s just super simple. And frankly, the other cool thing is when I go hunting or when I have long periods of time outdoors or when I’m at the beach and evening comes and I forgot my coat, I don’t get as bothered, which is just kind of nice. You’re just more tough.
[Damien Blenkinsopp]: It sounds like the only time it was an issue when you were doing you ketogenic thing. What was the issue there? Were you getting a lot colder, or?
[Ben Greenfield]: Yeah, but that was because of the thyroid. If you have hypothyroidism, cold thermogenesis is going to be very uncomfortable. Heck, even normal temperatures you’re colder during. So I was still doing cold thermogenesis then but it was quite unpleasant. It was hard for the body to get warm again.
[Damien Blenkinsopp]: Okay. Right, great.
[53:17] Some quick fly questions that I have just to finish off here.
First of all, if people want to connect with you and learn more about you and what you’re up to, where is the best place? Twitter, your website?
[Ben Greenfield]: Bengreenfieldfitness.com, because if you go there, you’ll find links to my Twitter, Facebook, Instagram, my blog, my podcast, etc. So that’s a good place to go as a portal.
[Damien Blenkinsopp]: Great, great. And who besides yourself would you recommend to learn more about endurance training, or some of the other topics we spoke about today? Ketogenic diets and so on?
[Ben Greenfield]: As far as people who have their head screwed on straight who are paying attention to the research, I’d say three people come to mind.
Number one would be Joe Friel. He’s coached a lot of professional cyclists, but also has just been in the sport a long time and pays attention to the science and the research and has a pretty good unbiased view of things.
Sami Inkinen, who is a top age group for Ironman competitor. He’s a higher fat diet, pays attention to quantified data, and is a smart, well spoken person who performs well.
And then Dr. Peter Attia, who I would not say is on the pointy edge of physical performance, even though he’s in much better shape than the average, general population. He’s not out doing Ironman triathlons or anything. But, as far as the science goes, he probably knows the science better than just about anybody else when it comes to being able to speak to these things, and he also does quite a bit of self-quantification himself.
So, those would be three people that would be good resources for this.
[Damien Blenkinsopp]: Great, thanks so much for that.
[54:48] Beyond everything, like all the biomarkers we’ve spoken about today, are there any other biomarkers you pay specific attention [to] on a routine basis, I don’t know whether it’s monthly that you feel are important that we haven’t spoken about?
[Ben Greenfield]: I’ll finish with this because it’s important. And many times in our type of circles it’s not talked about, and it’s not quantifiable to a great degree, as far as I know. And that would be simply paying attention to your levels of gratitude every single day, and multiple times per day.
For me, I guess you could kind of quantify it at least six times per day I’m grateful. Because I’m journaling, and at the beginning of the day I journal three things I’m grateful for, and at the end of the day I journal three amazing things that happened to me that day. So there’s at least six times per day that I’m being grateful for things.
And then I practice quick coherence technique, which is something you can read about at heartmath.org, which increases heart rate variability and decreases stress. And that’s where you simply think of something that you love or someone you hold dear, and you imagine intense feelings of gratefulness washing over your body and going into your heart after you feel those feelings of gratefulness.
Saying thank you to people, saying I love you to people, randomly calling up people and telling them how much you appreciate them. If you listen to my voicemail, I ask people to end their voice message by telling me one thing that they’re grateful for that day.
It’s certainly something that’s not super duper quantifiable, again, but it is one thing, not a biomarker, but certainly something I pay attention to every day is gratefulness for being alive, for the people in my life, for the experiences that I’ve had, and for simply being able to take one more breath.
[Damien Blenkinsopp]: Excellent. Thanks for that, that’s not the typical, but definitely something really important. So I can see how that would be useful. I do a meditation gratitude every morning too, and I find that really, really useful.
So Ben, thanks so much for your time today. It’s been really stock full of biomarkers and hacks and everything, so it’s really been a great episode. Thank you for your time.
[Ben Greenfield]: Awesome. Well thanks for having me on, Dam.